TL;DR
- Kegels work in theory and fail in practice. 30 to 50 percent of women cannot correctly isolate the pelvic floor muscle without biofeedback, per Bump et al. in the American Journal of Obstetrics and Gynecology. Voluntary contractions max out around 30 to 40 percent muscle fiber recruitment.
- Pelvic floor PT works if you do the homework. The Cochrane Database systematic review (Dumoulin et al., 2018) shows 50 to 75 percent symptom improvement, but benefits decline at 12 months without continued daily practice.
- Emsella delivers ~11,200 supramaximal contractions per 28-minute session. Samuels et al. (2019) in Lasers in Surgery and Medicine reported 95 percent quality-of-life improvement and 81.33 percent UI symptom reduction after 6 sessions.
- Surgery has the highest anatomical success rate (88 percent) and the highest complication rate (34.6 percent). Sacarin et al. (2025) compared anterior colporrhaphy directly against Emsella over 12 months.
- At 6 months post-treatment, 86.7 percent of Emsella patients vs 62.5 percent of PFMT patients showed improved pad use in head-to-head data.
- Emsella is FDA-cleared (510(k) K181497, November 2018) under 21 CFR 876.5320 as a Class II nonimplanted electrical continence device for male and female urinary incontinence.
- Recovery times are not even close. Surgery: 18.7 days. PFMT: ongoing. Kegels: ongoing. Emsella: 0 days. You walk out and go to lunch.
You have done the Kegels. You have read the pamphlet from your OB. You have laughed in a yoga class and felt the small betrayal that nobody warned you about. You have priced surgery, then closed the tab because the recovery time alone would cost you a season of your life.
So now you are sitting here trying to figure out: is Emsella actually different, or is it just the next thing on a list of things that did not work for you?
Fair question. The honest answer requires looking at all four options side by side, with real outcome data, real costs, and real recovery numbers. Not marketing copy. Not a brochure that promises "renewed confidence" without telling you what the trial endpoints were.
Here is the comparison, with citations.
The U.S. urinary incontinence treatment market exceeded $2.6 billion in 2024,
 Emsella vs Kegels: 11,200 supramaximal contractions per session
but the choices break down into exactly four real-world categories: home Kegels, supervised pelvic floor physical therapy (PFMT), HIFEM technology like Emsella, and surgery. Every other product or protocol is a variation on these four. Your decision is which trade-off you can live with.
Emsella vs Kegels: 11,200 supramaximal contractions per session
but the choices break down into exactly four real-world categories: home Kegels, supervised pelvic floor physical therapy (PFMT), HIFEM technology like Emsella, and surgery. Every other product or protocol is a variation on these four. Your decision is which trade-off you can live with.
Why Do Kegels Fail for So Many Women?
The most-prescribed pelvic floor intervention is also the most-failed. Not because the muscle group is wrong (it is not). Because the execution model is broken.
What's happening: Your doctor handed you a one-page sheet that says "tighten the muscle you would use to stop urinating, hold for 5 seconds, repeat 10 times, three times daily." You did it for 6 weeks. Nothing changed. You quietly stopped.
Why it fails: Three structural problems, all documented in the literature.
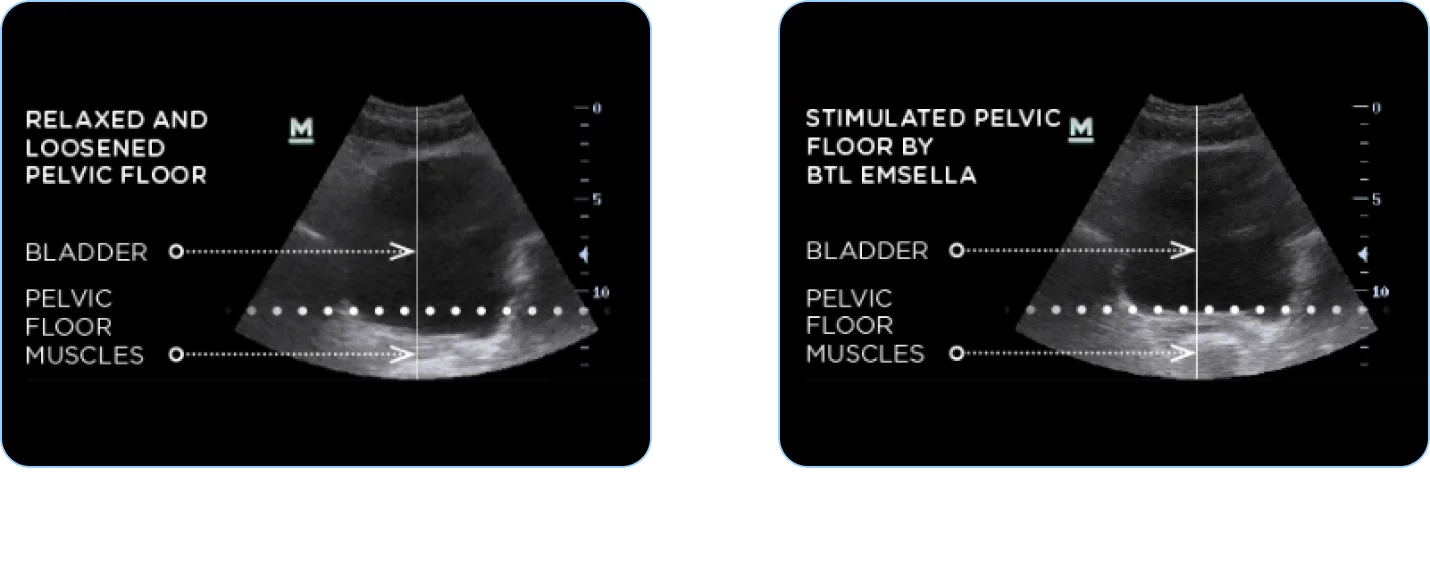 Pelvic floor anatomy, before and after Emsella treatment
Pelvic floor anatomy, before and after Emsella treatment
First, the technique problem. Bump et al. found that 30 to 50 percent of women cannot correctly isolate the levator ani without biofeedback confirmation. Many recruit gluteals, adductors, or abdominals instead. They are doing the exercise. They are not training the right muscle.
Second, the dose problem. Voluntary muscle contraction caps at roughly 30 to 40 percent of available muscle fibers. The pelvic floor needs supramaximal stimulation to remodel weakened or denervated tissue, especially after vaginal birth, menopausal estrogen decline, or chronic intra-abdominal pressure. A voluntary Kegel is a stretch at best.
Third, the adherence problem. Protocols typically require 60 to 100 contractions daily for 6 plus months before measurable change. Most women quit by week 8. The behavior is invisible (no one will notice you doing it), produces no immediate feedback, and competes with every other priority a busy life throws at it.
The fix: If Kegels are going to work for you, you need three things you probably do not have: a biofeedback device or pelvic PT to confirm correct muscle activation, a structured progressive overload protocol, and the discipline of a competitive athlete. Most women do not have all three at once. That is not a character flaw. It is a system mismatch.
Action Step: If you have done Kegels alone for more than 8 weeks with no measurable change, stop blaming yourself. The protocol is high-failure by design when delivered without supervision. Your next move is either supervised PFMT or a HIFEM device. Read the breakdown of Emsella patient acquisition cost and clinic economics to understand why clinics increasingly default to HIFEM as first-line.
How Does Pelvic Floor Physical Therapy Compare to Emsella?
PFMT is the closest cousin to Emsella in terms of mechanism (same target muscle, same goal: strength + neuromuscular coordination). The difference is dose precision and compliance burden.
What's happening: You see a pelvic floor PT for 12 sessions over 3 months. They use internal palpation, biofeedback, and supervised exercise progression. You also do daily homework between visits.
Why it fails (when it fails): The Cochrane systematic review (Dumoulin, Cacciari, Hay-Smith 2018) covering 31 trials and 1,817 women shows PFMT produces 50 to 75 percent symptom improvement when properly executed. That is real and meaningful. But three caveats matter.
The benefits decline at 12 months without continued daily practice. Adherence post-treatment hovers around 30 to 50 percent. And direct head-to-head data shows that at 6 months post-treatment, 86.7 percent of Emsella patients vs 62.5 percent of PFMT patients showed improved pad usage, per the comparative literature cited in BTL's clinical dossier.
The fix: If you have time, insurance coverage, and the discipline for daily home protocols, PFMT is genuinely effective and cheaper than Emsella. If you have already done PFMT and the gains plateaued or regressed, Emsella is the logical next step. The two are not enemies. Many clinics combine them.
Here is the head-to-head:
| Modality | Cost (cash) | Time investment | Recovery | Symptom improvement | Durability |
|---|---|---|---|---|---|
| Kegels (home) | $0 to $300 (biofeedback) | 60 to 100 reps daily, 6+ months | None | 30 to 40 percent (best case) | Drops off rapidly without adherence |
| Pelvic Floor PT | $1,200 to $2,000 | 12 sessions over 12 weeks + homework | None | 50 to 75 percent | Declines at 12 months without practice |
| Emsella (HIFEM) | $1,800 to $2,400 | 6 sessions over 3 weeks (28 min each) | 0 days | 81.33 percent UI reduction; 95 percent QoL improvement | 6 to 12 months + maintenance |
| Surgery (sling, anterior colporrhaphy) | $6,000 to $12,000 | 1 surgery + recovery | 18.7 days | 88 percent anatomical success | Permanent (with lifetime complication risk) |
Action Step: Ask yourself honestly: have you done daily home Kegels or PFMT homework for 8 plus weeks straight in the last year? If yes and it did not work, escalate to Emsella. If no, you have not actually tested PFMT. Try it first or accept the compliance reality and choose a passive intervention. For more on how clinics frame this conversation, see our Emsella objection handling playbook for the consult room.
Is Emsella Actually as Effective as the Marketing Claims?
Emsella's clinical evidence is the strongest in the non-surgical pelvic floor category. The numbers below come from peer-reviewed studies, not vendor brochures.
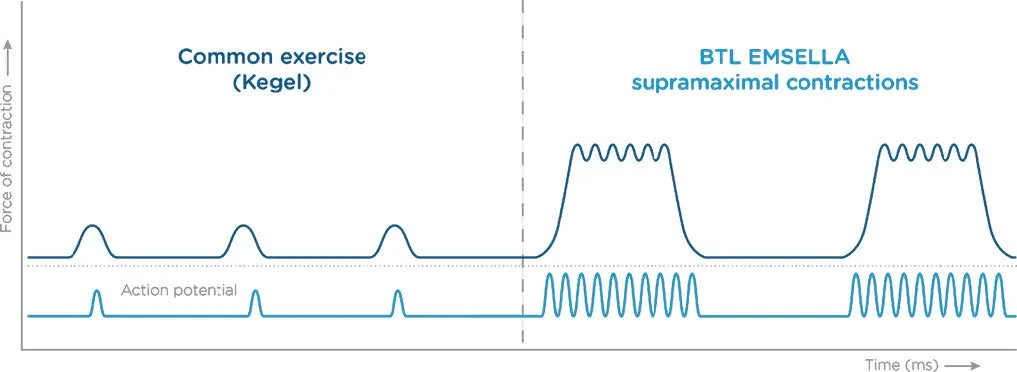
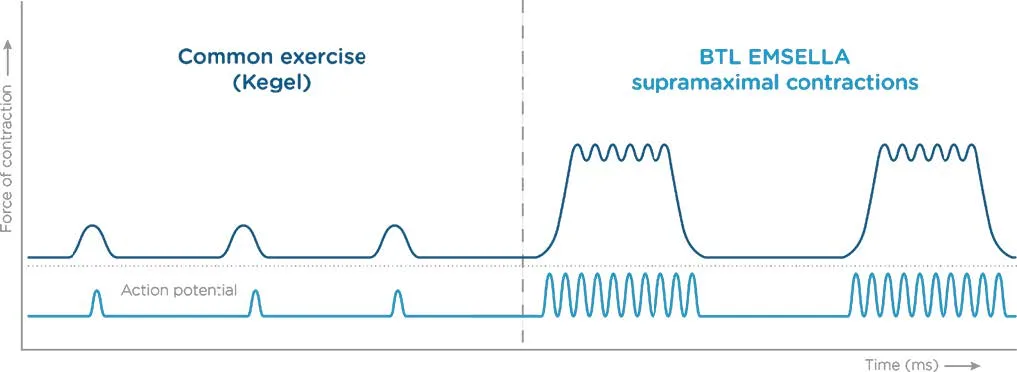
What's happening: A 28-minute session in a fully clothed seated position. The chair generates a focused electromagnetic field that triggers ~11,200 supramaximal pelvic floor muscle contractions per session. Six sessions over 3 weeks is the standard protocol.
Why it works (when it works): Samuels et al. (2019) published the foundational outcomes paper in Lasers in Surgery and Medicine (51:7, 760-766):
- 95 percent of patients reported improved quality of life after 6 sessions
- 75 percent reported significant pad usage reduction
- 81.33 percent reported significant UI symptom reduction
Silantyeva et al. (2021) in Female Pelvic Medicine and Reconstructive Surgery corroborated these findings in an independent cohort, with measurable urodynamic improvements and statistically significant patient-reported outcome gains.
The mechanism makes sense biomechanically. Voluntary Kegels recruit ~30 to 40 percent of muscle fibers. Emsella forces 100 percent recruitment via supramaximal HIFEM stimulation. You cannot match that intensity through your own nervous system. The muscle gets dosed at a level it would never see otherwise, then remodels in response.
The fix: This is not a magic chair. It is a high-dose neuromuscular re-education protocol that bypasses the technique and adherence problems that sink home Kegels and PFMT. The clinical evidence supports the marketing. The marketing usually understates the recovery numbers.
Action Step: Ask any prospective Emsella provider for their patient outcome data. If they cannot quote you their own clinic's pad-reduction or symptom-reduction percentages, find a different clinic. Real practitioners track results. For a deeper dive on what separates competent Emsella clinics from hobbyists, read our BTL Emsella clinic positioning guide for medspa, urology, and pelvic PT.
When Is Surgery Actually the Right Call?
Surgery is the highest-success and highest-cost option, with the longest recovery and the most permanent trade-offs. It is the right answer for some patients. It is the wrong answer when chosen by default.
What's happening: Your gynecologist or urogynecologist recommends a midurethral sling, anterior colporrhaphy, or related procedure. The pitch: definitive correction, insurance-covered after deductible, "one and done."
Why it sometimes fails (or shouldn't be first): Sacarin et al. (2025) ran a comparative study against Emsella with these reported endpoints:
- Anterior colporrhaphy: 88 percent anatomical success, 34.6 percent complication rate, 18.7 day average recovery, 14.1 percent dyspareunia (pain with intercourse)
- Emsella: 64 percent Stage 0 prolapse success, 0 percent dyspareunia, 2.3 day perceived recovery, no surgical complications
Surgery wins on raw anatomical correction, especially for advanced prolapse (Stage III to IV). But the 34.6 percent complication rate is not a footnote. It includes mesh erosion (in sling procedures), chronic pelvic pain, recurrent UTIs, and dyspareunia rates that materially affect intimate relationships for the rest of your life.
The FDA itself reclassified transvaginal mesh products in 2019 due to mounting adverse event data. The procedures still happen. They just are not the casual default they were 15 years ago.
The fix: Surgery is the right answer for severe prolapse (Stage III to IV), failed conservative treatment with significant quality-of-life impact, or specific anatomical defects like vesicovaginal fistula. It is the wrong answer as a first-line option for uncomplicated stress incontinence in a working mother who cannot lose 19 days. Try the non-surgical ladder first: PFMT, then Emsella, then surgery if needed.
Action Step: If a surgeon recommends surgery without first trialing PFMT or HIFEM, get a second opinion. Either from a pelvic floor PT, a urogynecologist who offers conservative options, or an Emsella provider. Surgical sequencing matters. You can always escalate up the ladder. You cannot un-do a sling.
What Does the Combined Recovery and Cost Math Actually Look Like?
The cost conversation almost always misses the recovery cost. A working mother who loses 18.7 days to surgery is not "saving money" relative to a $2,400 Emsella package, even if her insurance covers most of the surgery bill. Let us run the math.
What's happening: You compare the sticker prices: $0 for Kegels, $1,500 for PFMT, $2,100 for Emsella, $8,000 for surgery (assuming 80 percent insurance coverage post-deductible). Surgery looks expensive. Kegels look free.
Why this comparison fails: Sticker price ignores three real costs.
- Recovery time. At a $35/hour fully loaded wage, 18.7 days of surgical recovery is roughly $5,236 in lost wages or PTO. PFMT and Emsella are zero.
- Compliance time. Kegels demand 60 to 100 reps daily for 6+ months. At 5 minutes per session, that is 15+ hours of attention over half a year. Time has value.
- Failure cost. If a $0 Kegel protocol fails (and it does, 60 to 70 percent of the time per the literature), you have lost 6 months and now need to start a different intervention anyway. The "free" option had a real opportunity cost.
Real all-in cost comparison:
| Modality | Sticker | Recovery cost | Time cost | Failure-adjusted total |
|---|---|---|---|---|
| Kegels | $0 to $300 | $0 | 15+ hrs over 6 mo | $0 to $300 (60 to 70 percent fail rate) |
| Pelvic Floor PT | $1,200 to $2,000 | $0 | 24+ hrs over 12 wks | $1,200 to $2,000 (25 to 50 percent partial failure) |
| Emsella | $1,800 to $2,400 | $0 | 2.8 hrs total (6 sessions) | $1,800 to $2,400 (~5 to 19 percent non-response) |
| Surgery | $1,200 to $2,400 (post-insurance) | $5,200+ in lost wages | Surgical day + 18.7 days | $6,400 to $7,600 (12 percent fail to achieve goal, 34.6 percent complication risk) |
The fix: Choose based on your real constraints, not the sticker price. If your time is worth nothing and you have full daily discipline, do Kegels first. If you have insurance and patience, do PFMT. If you have $1,800 to $2,400 cash and want a high-probability passive intervention with zero recovery, do Emsella. If you have severe prolapse and have already failed conservative treatment, surgery is your answer. The math is personal. The data is universal.
Action Step: Calculate your own all-in cost using your hourly wage, your insurance situation, and your time tolerance. If Emsella's clinic-stated cost is unclear, our Emsella ROI and payback period guide breaks down the typical $1,800 to $2,400 package economics and what is included.
Who Is the Best Candidate for Each Option?
Not every modality fits every patient. Here is the honest matching grid.
Best candidates for Kegels alone:
- Mild stress incontinence, postpartum first 6 weeks
- Confirmed correct muscle activation via biofeedback or PT assessment
- High personal discipline + no immediate quality-of-life impact
Best candidates for Pelvic Floor PT:
- Moderate stress, urge, or mixed incontinence
- Insurance coverage available
- Patient willing to commit to 12 weeks of supervised + home protocol
- Pelvic pain, prolapse Stage I to II, postpartum diastasis recti
Best candidates for Emsella:
- Failed Kegels or PFMT
- Stress, urge, or mixed incontinence (Stage 0 to II)
- Post-prostatectomy male incontinence (often overlooked)
- Patients who cannot or will not commit to daily home protocols
- Working professionals who need zero recovery
- No metal implants, pacemaker, copper IUD, or pregnancy
Best candidates for Surgery:
- Stage III to IV prolapse
- Failed conservative treatment with significant quality-of-life impact
- Specific anatomical defects (fistula, severe rectocele, etc.)
- Patient prepared for 18+ day recovery and 34.6 percent complication risk
The fix: Most patients should try the ladder in order: Kegels (with biofeedback confirmation), then PFMT, then Emsella, then surgery if needed. Most clinicians skip rungs because of practice incentives or training bias. Be your own advocate.
Action Step: Bring this candidate grid to your next appointment. If your provider cannot explain why they are skipping a rung of the ladder for your specific case, ask. Sequencing matters more than any single intervention. For the broader picture of how Emsella fits inside a multi-device clinic strategy, read our Emsella vs Emsculpt vs Emface service mix analysis.
What Is the Honest Bottom Line?
There is no single winner. There is a sequencing question, and there is a personal-constraints question.
If you have done nothing yet: Start with biofeedback-confirmed Kegels or 12 sessions of PFMT. Real, measurable, low-cost.
If you have done Kegels or PFMT and plateaued: Emsella is the logical next step. Six sessions, 28 minutes each, FDA-cleared, ~80 percent symptom improvement in published data, zero recovery.
If you have severe prolapse or have failed conservative treatment: Surgery, with full understanding of the 34.6 percent complication rate and 18.7 day recovery.
If you are post-prostatectomy: Emsella is undermarketed and clinically supported. Ask.
The patients who suffer longest are the ones who think the choice is binary: free Kegels or expensive surgery. There are two well-validated middle steps that most women never get offered. The 6.5 year average delay from incontinence onset to seeking professional help is not because the conditions are mysterious. It is because the system rarely presents the full ladder.
Now you have it.
If you run an Emsella clinic and want help positioning your service against Kegels, surgery, and pelvic floor PT in your local market, book a free Emsella growth strategy call and we will map your messaging, your consult flow, and your competitive positioning before we ever quote a service.
Read Next
- Emsella Sales Objection Handling: Close the $2,400 Package - How clinics handle the price, fear, and skepticism conversations
- Emsella vs Emsculpt vs Emface: Which Mix Maximizes Revenue? - Service mix strategy for clinics offering multiple BTL devices
- Emsella Positioning: MedSpa vs Urology vs Pelvic PT - Why the same device wins different patients in different clinic verticals